MEDIMAGE 701 Imaging Anatomy and Pathology Assignment - The University of Auckland, New Zealand
Assignment Title - Hypothetical study Acute Cholecystitis
Question - Select a non-oncological pathology of your choice (excluding liver conditions), for which a minimum of two (2) different imaging modalities may be used for diagnosis. Prepare a written case study explaining the preliminary clinical course of a hypothetical patient who presents to your department with this particular pathology.
ORDER NEW MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT & GET 100% ORIGINAL SOLUTION AND QUALITY WRITTEN CONTENTS IN WELL FORMATS AND PROPER REFERENCING.
Answer - Introduction of the Patient and Case
Case Identified
Disease: Acute Cholecystitis
Case Presentation
Signs and symptoms
The patient is a 48 years old woman who has presented the symptoms of right upper quadrant (RUQ) pain. The patient woke up at 1 am with the sudden onset progressive pain and perfuse vomiting for about 3 hours and had an aching pain in RUQ radiating towards the back. She had feelings of hot and cold overnight and an ultrasound confirmed the presence of acute cholecystitis with gallstones.
Indication
Known gall stone history and with 1-day history of sudden onset of RUQ pain as well vomiting. The CRP was 11, WCC was 12.1. Murphy's was positive on exam. Cholecystitis possibility?
Findings
- The liver is normal in the echotexture with no focal hepatic lesion identified.
- The portal vein measures 8 mm in diameter and demonstrates hepatoportal flow.
- The gallbladder is thick-walled, up to 13 mm and contains multiple gallstones. There is a non-mobile gallstone at the gallbladder neck. The patient was tender to probe pressure over the region of the gallbladder. No intra-hepatic biliary dilation, CBD = 5 mm (the distal CBD at the pancreatic head is not well visualized).
- Normal pancreas. No pancreatic duct dilation.
- The spleen measures 9 cm in length.
- Normal calibre aorta. Normal right kidney. The left kidney was not well visualized; no abnormality detected. The right kidney measures 11.7 cm in length and the left kidney 11.8 cm.
- No free fluid.
GET GUARANTEED SATISFACTION OR MONEY BACK UNDER MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT HELP SERVICES OF EXPERTSMINDS.COM - ORDER TODAY NEW COPY OF THIS ASSIGNMENT!
Interpretation
The findings are in coherence with acute calculous cholecystitis and no biliary tract dilation.
History of the present illness: The patient is a 48 years old female with the history of aortic arch that is secondary to the invasive aspergillosis, with an addition to the known history of gallstones have been admitted to the emergency department, who has been experiencing right upper quadrant pain, along with vomiting, nausea and fiver for the past two days.
Significant findings: The vitals of the patients were in coherence with tachycardia and the physical examinations were notable for a positive Murphy's sign. The initial lab results detailed significant presence for leukocytosis with an elevated level of alkaline phosphatase. Furthermore, point of care ultrasounds revealed the presence of a distended gallbladder, with thickened walls and presence of pericholecystic fluid and a stone that was present in the neck of the gallbladder that was indicative of acute cholecystitis.
Discussion: The prevalence of gallstones is high in the western nations and they typically cause intermittent abdominal pain within the right upper quadrant, which worsens after eating, and this condition is known as biliary colic. The patients with acute cholecystitis typically present with similar kind of pain as that of biliary colic and often endorses nausea, low grade fever, vomiting, leukocytosis and anorexia (Chad & Lindsey, 2018).
Normal Anatomy
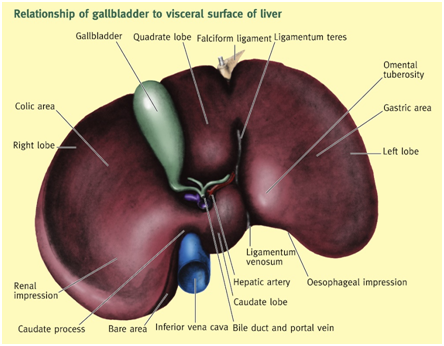
The gallbladder is fundamentally a thin, and elongated sac that is about 8 cm and comprises of 50 mL in volume that is present at the fossa on the inferior surface of the liver between the quadrate and right lobes. It fundamentally originates from the same foregut diverticulum that eventually produces liver. The primary function of gallbladder includes rise, concentration and storage of bile. The cystic duct of gallbladder is nearly 3 cm long and it drains the gallbladder inside the hepatic duct. The duct comportments dilute bile into the gallbladder from the hepatic duct, whereby it concentrates and eventually gets discharged to the common bile duct (Strayer, Rubin, Saffitz & Schiller, 2015).
Gallbladder's wall comprises of mucous membrane, an adventitia and a muscularis. It is fundamentally covered by a reflection of visceral peritoneum. Into the walls, dips the Rokitansky-Aschoff sinuses mucosal diverticulum. The mucosa of gallbladder comprises of columnar epithelium, along with a lamina propria of loose connective tissue.
DO WANT TO HIRE TUTOR FOR ORIGINAL MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT SOLUTION? AVAIL QUALITY MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT WRITING SERVICE AT BEST RATES!
Figure: Schematic view of the interior of gallbladder and the extrahepatic biliary duct
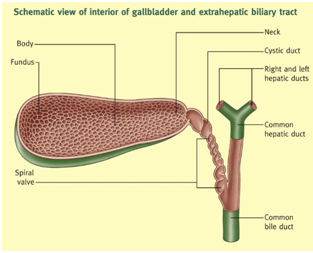
The gallbladder is further divided into fundus body and neck, which opens into the cystic duct. This is the rounded end that projects beyond the anterior margin of the liver's visceral surface and is present behind the tip of the 9th costal cartilage (Mahadevan, 2014). The body and neck are supermedially directed towards the porta hepatis. Under pathological conditions, on the ventral facet of the organ, a pouch is present frequently, just proximal to the neck. Within this lies an impacted or solitary collection of calculi which is termed as Hartmann's pouch (Ellis, 2010).
Figure: Relationships of gallbladder to visceral surface of liver
Pathological Process
Pathophysiology
About 90% of the individual with gallstone account for acute cholecystitis. The restare associated with severe trauma, sepsis, polyarteritis nodosa along with infection of the gallbladder with Salmonella typhosa. Bacterial infections are usually consequence of the biliary obstruction, rather than any primary event. The obstruction by gallstone of the cystic duct results in the release of phospholipase by the gallbladder epithelium. This enzyme causes hydrolysis of lecithin to lysolecithin, which is a membrane active toxin. The mucous coat is disrupted that exposes the mucosal cells and is subjected to the detergent action of the concentrated bile salts. Furthermore, bile that is supersaturated with cholesterol can be toxic to the epithelium layers (Strayer, Rubin, Saffitz, & Schiller, 2015).
Pathogenesis
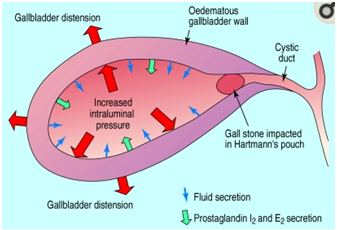
In more than 90% of the cases, acute cholecystitis occurs majorly due to the obstruction of the cystic duct by the gall stones or due to the biliary sludges that gets wedged at the neck of the gall bladder. The obstruction of the cystic duct results in the rise of intraluminal pressure inside the gallbladder and along with cholesterol supersaturated bile, it activates an acute inflammatory response. The resultant trauma further stimulates the prostaglandins I2 and E2 synthesis that eventually mediates the inflammatory response. In about 20% of the cases, a secondary bacterial infection with enteric organisms such as Streptococcus faecalis, Klebsiella, and Escherichia coli, occurs. If the biliary sludge, which is primarily a mixture of bile and particulate matter that stimulates microlithiasis, persists, the formation of gallstones take place. This is further facilitated due to multiple pregnancies or amongst recipients of parenteral nutrition. Majority of patients with biliary sludges present no symptoms, however, the sludge itself causes acute cholecystitis (Indar & Beckingham, 2002).
GETTING STUCK WITH SIMILAR MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT? ENROL WITH EXPERTSMINDS'S MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT HELP SERVICES AND GET DISTRESSED WITH YOUR ASSIGNMENT WORRIES!
Figure: Gallstone formation
Pathophysiology
In cases of acute cholecystitis, the exterior surface of the gallbladder is layered and congested with a fibrinous exudate. The wall thickens due to edema and the mucosa becomes purple or fiery red. The gallstones are generally present in the lumen and is found to obstruct the cystic dust. In certain cases, in empyema of the gallbladder, there occurs complete obstruction of the cystic duct, which allows the bacteria to invade into gallbladder, thereby causing distension of the organ, along with purulent and cloudy fluid formation. Inside the walls of gallbladder, there occurs hemorrhage and edema that is accompanied by chronic and acute inflammation. Suppuration in the wall is followed by bacterial invasion. In most cases, the mucosa presents focal ulcers and in severe cases results in widespread necrosis or gangrenous cholecystitis. In many cases, perforations occur, and the bile leakage reaches the peritoneum, thereby causing bile peritonitis. More often, the inflammatory adhesions result in the formation of pericholecystic abscess and limits the spread of the gallbladder contents after the perforations. The erosion of the contents of gallbladder into a viscus results in the creation of a cholecystentric fistula (Strayer, Rubin, Saffitz, & Schiller, 2015).
Figure: Acute cholecystitis
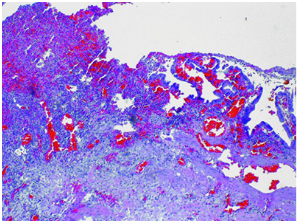
The presented image is a gallbladder that has been removed from a patient with acute cholecystitis thereby demonstrating ulceration of the mucosa, along with chronic and acute inflammation.
Histological changes
The presence of transmural and mucosal infiltrates of a wide range of polymorphonuclear neutrophils (PMNs) with alterations of the mucosa such as hemorrhage and necrosis. The gallbladder wall exhibits necrotic that has resulted from acute inflammatory process.
Clinical manifestation
The prevalence of acute cholecystitis has been observed at a rate of 3% amongst the western societies and more than 500,000 annual cholecystectomies are performed each year in the United States. Most of the patients belong to the age ranges of 40 to 80 years and majority of the men present biliary colic along with acute cholecystitis. Due to the presence of stone being high amongst females, there are more females suffering from acute cholecystitis. The ratio of female and males is estimated to be about 3:1.
ORDER NEW COPY OF MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT AND SECURE HIGHER MARKS!
The patients generally exhibit RUQ or epigastric colic which persists or escalates over a period of 12 to 24 hours. It cannot be completely resolving, although may be ameliorated by analgesia administration. Generally, the patients with history of milder to escalated antecedent episodes of biliary colic may be present. The other obvious symptoms include nausea, anorexia, vomiting, malaise and chills. The examiner is required to ensure that the patient is questioned regarding clay clored stools or icteric orange-tea colored urine that raises the suspicion of common duct obstruction. Physical examination presents that the patient has low to moderate fever, marked RUQ tenderness and tachycardia. The following flowchart details the rest of the details regarding the clinical manifestations.

Imaging Appearances of the Pathology
Ultrasound
Ultrasound is commonly used for initial imaging in suspected cases of acute cholecystitis, on the basis of the clinical features. Ultrasound presents the specificity and sensitivity of 81% and 82%, respectively, in the diagnosis of acute cholecystitis (Katabathina, Zafar, & Suri, 2015). Ultrasound findings support presence of acute cholecystitis due to gallbladder distension of more than 4 cm, along with thickened wall of more than 3 mm. sludge or gallstones demonstration of a nonmobile store wedged in the neck of gallbladder is observed, along with hyperemia of the walls and hyper echogenicity of pericholecystic fat, that are shown by color Doppler. Ultrasound findings also include Murphy's sign that comprises of pain that are elicited by transducers pressure on the hypochondrium of the patient during the exploration (Volpacchio, Moras, Rubio, & Santamarina, 2012). The findings are as follows.
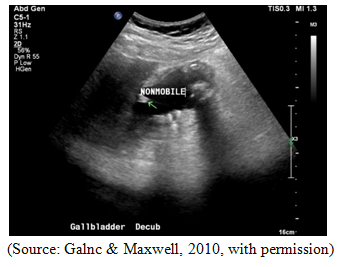
There are present multiple gallstones with a stationary gallstone at the neck of the gallbladder. No intrahepatic biliary dilation has been observed. The distal CBD is not seen, while the CBD is 3 mm. Ultrasonography is considered as the first test to diagnose the acute cholecystitis as it is specific, inexpensive, sensitive, rapid and has no adverse impact.
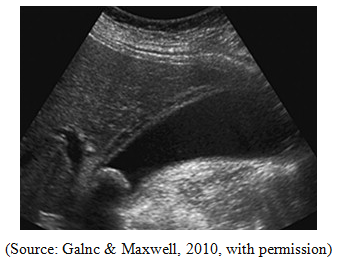
From the image it is evident that sagittal sonogram presents a single calculus wedged in the gallbladder neck. The additional findings include striated wall thickening and mildly distended gallbladder.
Computed Tomography Scanning (CT Scan)
CT scan of acute cholecystitis encompasses abnormal distension of gallbladder, mucosal or mural hyperenhancement and cholelithiasis, with edema and wall thickening, along with the presence of soft tissue stranding and pericholecystic fluid.


The CT scan evaluation plays a significant role in the assessment of the complications such as hepatic abscess and perforation (Volpacchio, Moras, Rubio, & Santamarina., 2012). Furthermore, through the CT scans, gallstones may be visualized dependent on the size and composition of the gallstones, however, the existence of gallstones may exhibit in the nonappearance of acute cholecystitis (Eachempati & Reed, 2015).
NEVER BE CAUGHT IN PLAGIARISM, AVAIL MEDIMAGE 701 IMAGING ANATOMY AND PATHOLOGY ASSIGNMENT HELP SERVICE OF EXPERTSMINDS.COM AND SAVE HIGHER MARKS!
Lists of courses of The University of Auckland, New Zealand which are covered under our Assignment Help service:-
- MEDIMAGE 702 Professional Issues in Medical Imaging Assignment Help
- MEDIMAGE 707 Mammographic Technology Assignment Help
- MEDIMAGE 708 Nuclear Medicine Technology Assignment Help
- MEDIMAGE 710 CT Imaging Technology Assignment Help
- MEDIMAGE 711 Musculoskeletal Trauma Image Evaluation Assignment Help
- MEDIMAGE 712 Musculoskeletal Pathology Image Evaluation Assignment Help
- MEDIMAGE 714 Fundamentals of Clinical MRI Assignment Help
- MEDIMAGE 715 MRI Technology Assignment Help
- MEDIMAGE 716 Fundamentals of Clinical Ultrasound Assignment Help
- MEDIMAGE 717 Ultrasound Imaging Technology Assignment Help
- MEDIMAGE 718 Acute Chest Image Evaluation Assignment Help
- MEDIMAGE 719 Paediatric Image Evaluation Assignment Help
- MEDIMAGE 720 Fundamentals of Clinical Nuclear Medicine Assignment Help
- MEDIMAGE 721 MRI Safety Assignment Help